By Prabakar Mahalingam, Managing Partner, AED Total Solution
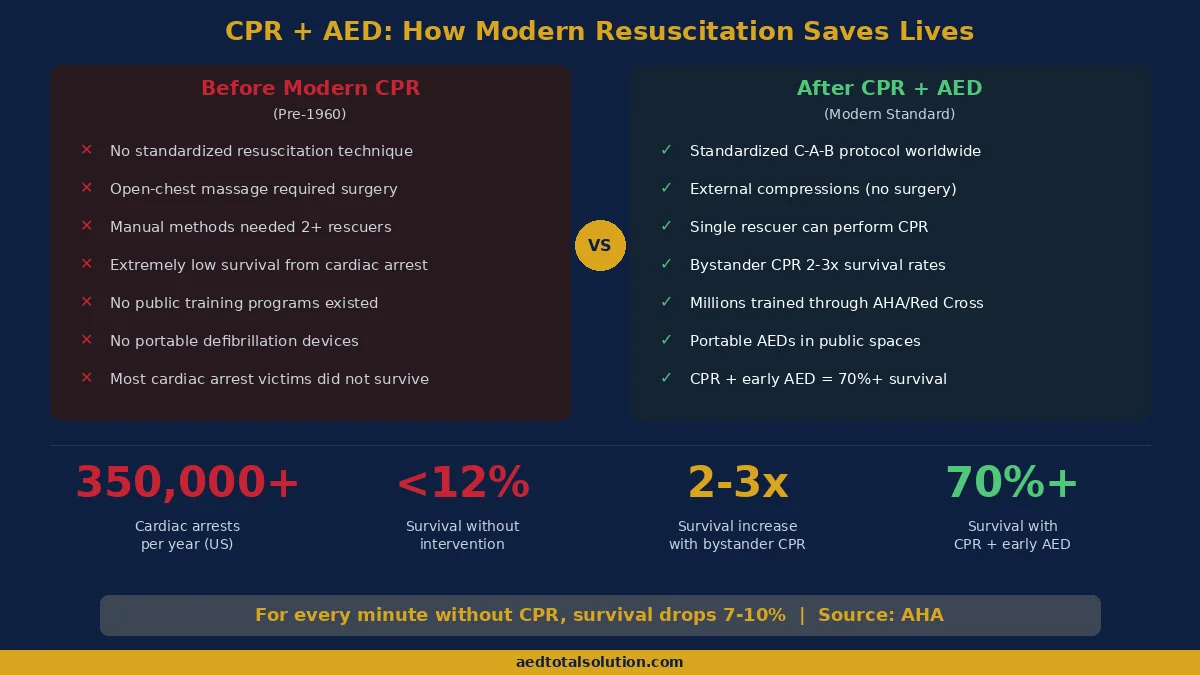
CPR, or cardiopulmonary resuscitation, is one of the most important lifesaving techniques ever developed. Every year, more than 350,000 Americans experience out-of-hospital cardiac arrest, and CPR performed by a bystander can double or triple survival rates. But who invented CPR, and how did it become the emergency standard we rely on today?
The answer involves centuries of medical experimentation and three pioneering physicians who, in 1960, combined chest compressions with rescue breathing to create modern CPR. This article traces the complete history of cardiopulmonary resuscitation, from ancient techniques through the breakthroughs that shaped emergency medicine.
Ancient Origins of Resuscitation
The concept of reviving an unconscious person dates back thousands of years. Ancient Egyptian texts describe the goddess Isis breathing life into her husband Osiris. In the first century AD, the Greek physician Galen described blowing air into the lungs of a deceased animal using a reed, one of the earliest documented attempts at artificial ventilation.
These ancient methods were rudimentary, but they reflected an understanding that breath was essential to life. For centuries, healers across civilizations experimented with ways to restore breathing in drowning victims, suffocation cases, and other emergencies.
Get certified in CPR

CPR & AED Training
3-hour in-person training with a 2-year nationally recognized certification.
CPR, AED & First Aid Certification
Instructor-led on-site. Practice on real manikins and AED trainers.
Early Artificial Respiration (1500s-1700s)
The scientific foundation for resuscitation began taking shape during the Renaissance. In the 1530s, Swiss physician Paracelsus used fireplace bellows to push air into the nostrils of patients who had stopped breathing. Around the same time, Andreas Vesalius described inflating the lungs of animals through a tube inserted into the trachea.
A major milestone came in 1740, when the Paris Academy of Sciences officially recommended mouth-to-mouth resuscitation for drowning victims. This was one of the first formal endorsements of a resuscitation technique by a scientific body.
In 1767, the Society for the Recovery of Drowned Persons was established in Amsterdam. It was the first organized group dedicated to developing and teaching resuscitation methods. Their techniques included warming the body, positioning the patient, and attempting to force air into the lungs.
The 19th Century: Chest Compressions Emerge
The 1800s brought significant advances in understanding how the heart and lungs work together. Researchers began experimenting with mechanical methods to circulate blood and restore breathing.
In 1891, Dr. Friedrich Maass performed the first documented external chest compressions on a human patient. He successfully revived a person who had suffered cardiac arrest during surgery. This was a breakthrough moment, demonstrating that pressing on the chest could manually pump blood through the body.
In 1903, Dr. George Crile became the first American physician to successfully use external chest compressions to resuscitate a patient. His work with animal experiments proved that external pressure on the chest could restart circulation, reinforcing Maass’s earlier findings.
During this period, several manual methods of artificial respiration were also developed, including the Silvester method (arm-lifting technique) and later the Holger-Nielsen method, which combined chest pressure with arm movements to force air in and out of the lungs. The Holger-Nielsen technique became widely used during World War II.
Who Invented CPR? The Three Pioneers of Modern CPR
Modern CPR was not the work of a single person. It was developed through the combined efforts of three physicians in the late 1950s and 1960:
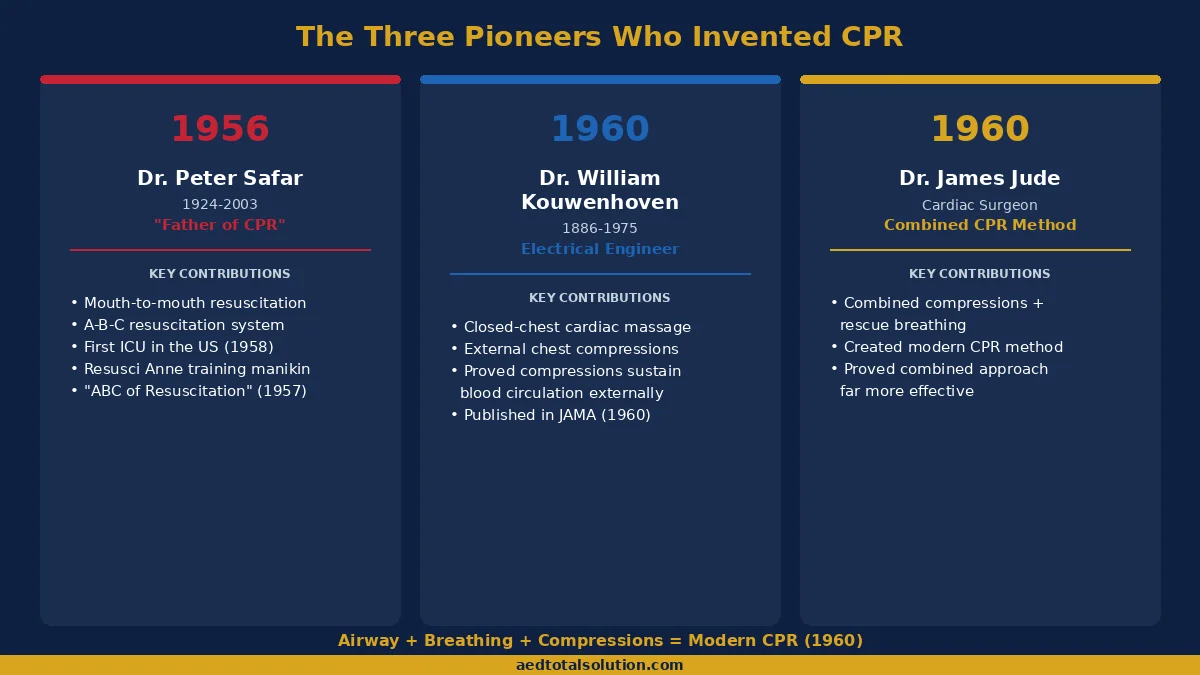
Peter Safar: The Father of CPR
Dr. Peter Safar (1924-2003), an Austrian-born anesthesiologist, is widely recognized as the “father of CPR.” Working at Baltimore City Hospital starting in 1956, Safar conducted groundbreaking experiments demonstrating that mouth-to-mouth breathing by a rescuer could maintain adequate oxygen levels in a non-breathing patient.
Together with Dr. James Elam, who had proven in 1954 that expired air contained enough oxygen to sustain life, Safar developed the mouth-to-mouth resuscitation technique. Safar then created the A-B-C system: Airway, Breathing, and Circulation. He published the book “ABC of Resuscitation” in 1957, which became the foundation for CPR training worldwide.
Safar also influenced Norwegian toymaker Asmund Laerdal to create “Resusci Anne” (also known as CPR Annie), the first CPR training mannequin. This training tool made it possible to teach CPR techniques to the general public on a large scale.
Beyond CPR, Safar established the first intensive care unit (ICU) in the United States in 1958 at Baltimore City Hospital and later founded the International Resuscitation Research Center at the University of Pittsburgh.
William Kouwenhoven: Closed-Chest Cardiac Massage
Dr. William Kouwenhoven (1886-1975) was an electrical engineer and researcher at Johns Hopkins University. While studying defibrillation in the 1950s, Kouwenhoven and his team, including research engineer Guy Knickerbocker and cardiac surgeon James Jude, made a critical discovery: applying rhythmic pressure to the chest could maintain blood circulation without opening the chest cavity.
This technique, called closed-chest cardiac massage, was a major advancement over open-chest massage, which required surgery. Their research, published in the Journal of the American Medical Association in 1960, demonstrated that external chest compressions alone could sustain circulation long enough for a patient to receive definitive care.
James Jude: Combining Compressions with Ventilation
Dr. James Jude, a cardiac surgeon working alongside Kouwenhoven, recognized that chest compressions alone were not enough. Patients also needed ventilation to maintain oxygen levels in the blood. By combining Kouwenhoven’s closed-chest compressions with Safar’s mouth-to-mouth breathing technique, the three physicians created what we now know as CPR.
In 1960, the combination of chest compressions and rescue breathing was formally introduced. This was the birth of modern cardiopulmonary resuscitation.
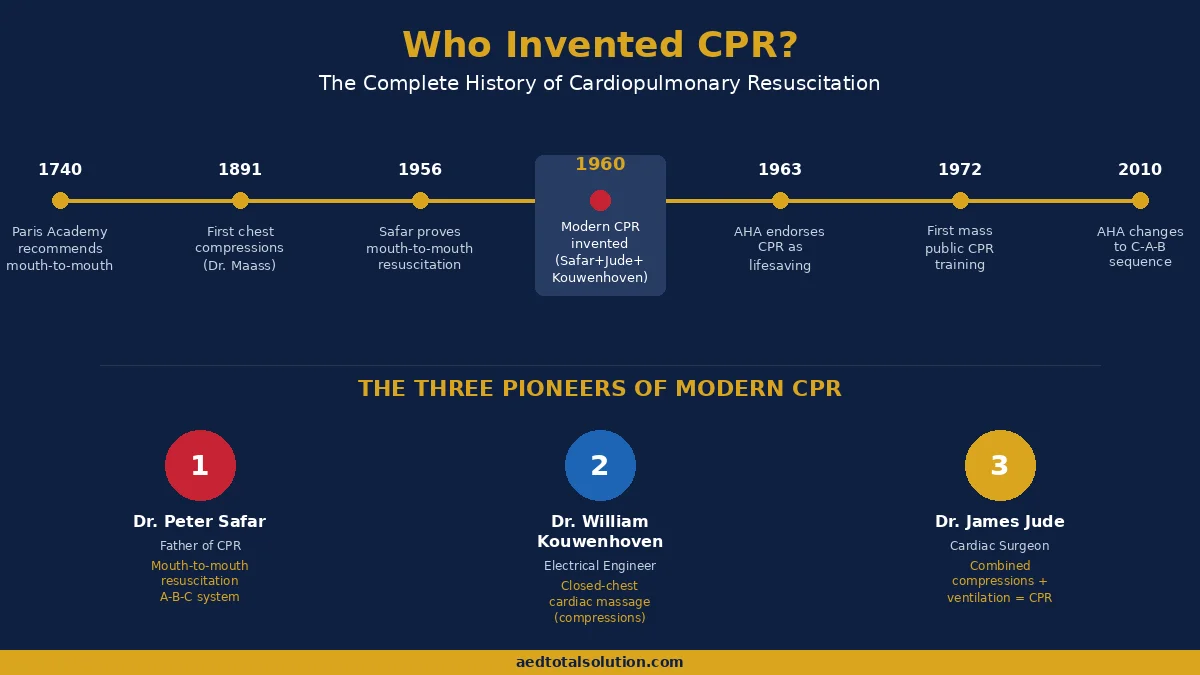
When Was CPR Invented? A Timeline
Understanding the full history of CPR requires looking at key milestones spanning centuries:
| Year | Milestone |
|---|---|
| 1740 | Paris Academy of Sciences recommends mouth-to-mouth for drowning victims |
| 1767 | Society for Recovery of Drowned Persons founded in Amsterdam |
| 1891 | Dr. Friedrich Maass performs first documented external chest compressions |
| 1903 | Dr. George Crile achieves first successful closed-chest resuscitation in America |
| 1954 | James Elam proves expired air maintains adequate oxygen levels |
| 1956 | Peter Safar demonstrates mouth-to-mouth resuscitation at Baltimore City Hospital |
| 1957 | Safar publishes “ABC of Resuscitation”; US military adopts mouth-to-mouth |
| 1958 | Safar establishes first ICU in the United States |
| 1960 | Modern CPR invented by combining compressions + ventilation (Safar, Kouwenhoven, Jude) |
| 1960 | AHA starts physician CPR training program |
| 1963 | AHA officially endorses CPR as a lifesaving technique |
| 1966 | National Research Council holds landmark conference on CPR standards |
| 1972 | First mass public CPR training (Medic 2 program in Seattle, led by Dr. Leonard Cobb) |
| 1973 | AHA publishes first official CPR standards and guidelines |
| 1981 | First automated external defibrillators (AEDs) developed for public use |
| 2000s | AHA updates guidelines to emphasize high-quality CPR and AED integration |
| 2010 | AHA changes CPR sequence from A-B-C to C-A-B (Compressions first) |
RECOMMENDED
HeartSine Samaritan 350P AED Package
Compact, fully-automatic AED designed for first-time responders. Pads, battery, carry case and wall sign included.
How CPR Training Became Widespread
After the AHA endorsed CPR in 1963, the focus shifted to making this technique accessible to everyone, not just medical professionals.
In 1966, the National Research Council convened a landmark conference that established standardized CPR training protocols. This led to the creation of formal training courses that could be taught to the general public.
A pivotal moment came in 1972, when Dr. Leonard Cobb organized the world’s first mass CPR training program in Seattle, called Medic 2. This initiative trained over 100,000 citizens in CPR, demonstrating that ordinary people could learn and effectively perform lifesaving resuscitation. The success of the Seattle program became a model for community CPR training programs nationwide.
The development of the Resusci Anne training mannequin made hands-on practice possible in classrooms, workplaces, and community centers. Combined with the AHA’s 1973 publication of official CPR standards, these efforts transformed CPR from a medical procedure into a public skill.
Today, organizations like the AHA and the American Red Cross continue to update CPR guidelines and offer CPR certification courses to millions of people each year.
From CPR to CPR + AED: The Modern Standard
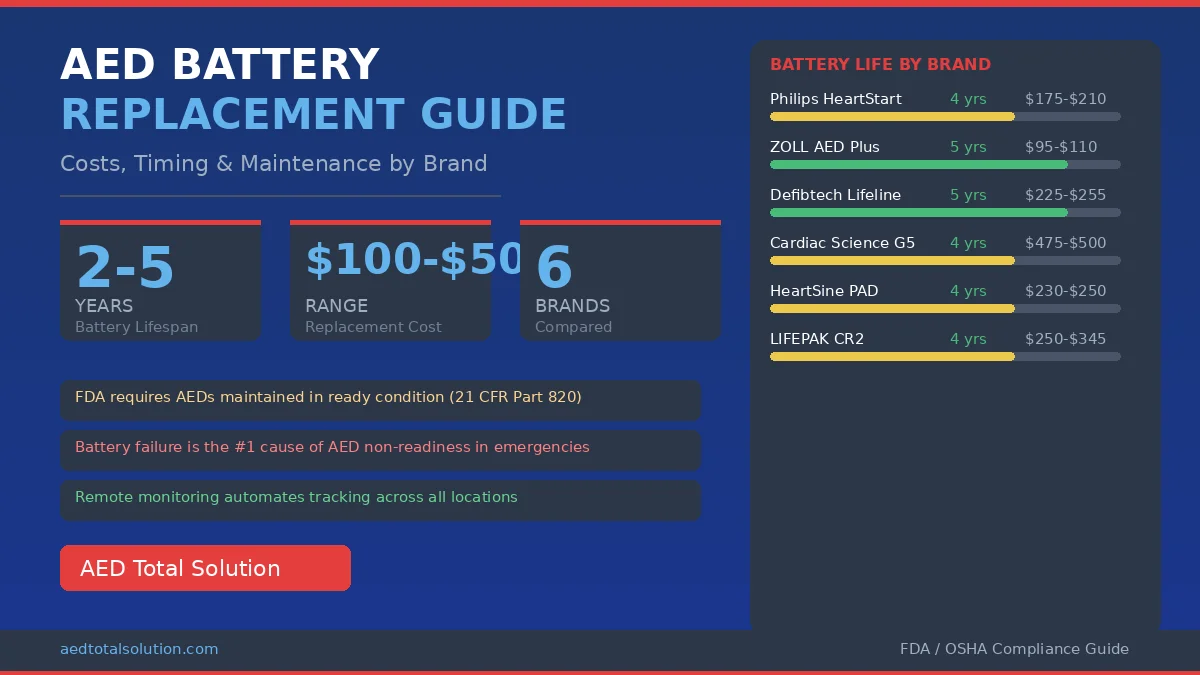
The invention of CPR was a turning point in emergency medicine, but the integration of automated external defibrillators (AEDs) in the 1980s and 1990s took cardiac arrest survival to the next level.
CPR alone maintains blood flow and oxygen delivery to the brain and vital organs, but it cannot correct the abnormal heart rhythm (ventricular fibrillation) that causes most cardiac arrests. AEDs analyze the heart’s electrical activity and deliver a controlled shock to restore a normal rhythm.
Research shows that performing CPR combined with early AED use within the first few minutes of cardiac arrest can increase survival rates to over 70%, compared to less than 12% for out-of-hospital cardiac arrest without intervention. This is why modern CPR guidelines emphasize the “Chain of Survival”: early recognition, early CPR, early defibrillation, and advanced medical care.
For organizations managing AED programs, ensuring that both CPR training and AED readiness are maintained is essential. Proper AED program management covers device maintenance, compliance documentation, and staff training to ensure your team is prepared when seconds count.
CPR in 2026: Latest Guidelines and Best Practices
CPR techniques continue to evolve based on new research. The latest 2025 AHA guidelines emphasize several important updates that every trained responder should know:
- Compression-first approach (C-A-B): Start chest compressions immediately before opening the airway or delivering breaths. This ensures blood flow to the brain begins within seconds.
- Hands-only CPR for bystanders: Untrained bystanders should perform hands-only CPR (continuous chest compressions at 100-120 per minute) rather than delay action trying to give rescue breaths.
- AED use within 3-5 minutes: The emphasis on early defibrillation with an AED has intensified. Every workplace, school, and public facility should have an accessible, maintained AED.
- Compression depth of 2-2.4 inches: Push hard and fast on the center of the chest, allowing full chest recoil between compressions.
- Minimize interruptions: Pauses in chest compressions should be less than 10 seconds. Switch compressors every 2 minutes to prevent fatigue.
How Modern CPR Training Has Evolved
Today, CPR training is more accessible than ever. The American Heart Association, American Red Cross, and many private organizations offer both in-person and blended learning CPR and AED certification courses. Key developments include:
- Compression-only training: Simplified courses focused solely on chest compressions, making it easier for non-medical professionals to learn.
- AED integration: Modern CPR courses always include AED training, teaching students how to use automated external defibrillators alongside compressions.
- Pediatric-specific protocols: Updated techniques for infants and children, including modified compression depths and the importance of pediatric AED pads.
- Workplace CPR requirements: Many states now require AED programs and CPR-trained staff in workplaces, schools, and public buildings.
Why CPR and AED Together Save More Lives
While CPR alone maintains blood flow to vital organs, it cannot correct the underlying heart rhythm problem. In approximately 70% of out-of-hospital cardiac arrests, the initial rhythm is ventricular fibrillation — a chaotic electrical disturbance that only defibrillation can correct.
This is why organizations invest in comprehensive AED program management: having an AED on-site and a team trained in both CPR and AED use creates the best possible outcome for cardiac arrest victims. With proper compliance management, your AEDs are always inspected, pads are current, and batteries are charged.
CPR Facts You Should Know
- More than 350,000 out-of-hospital cardiac arrests occur in the US each year (AHA).
- Bystander CPR can double or triple survival rates after cardiac arrest.
- The survival rate for out-of-hospital cardiac arrest is less than 12% nationally.
- For every minute without CPR or defibrillation, survival chances drop by 7-10%.
- Only about 46% of out-of-hospital cardiac arrest victims receive bystander CPR.
- Pediatric CPR requires modified techniques for infants and children.
- CPR certification typically needs to be renewed every two years.

Not sure which AED or program fits your facility?
An AED Total Solution program expert walks you through it — no obligation.
FAQ: Who Invented CPR?
Who invented CPR?
Modern CPR was developed in 1960 through the combined work of three physicians: Dr. Peter Safar, who developed mouth-to-mouth resuscitation; Dr. William Kouwenhoven, who pioneered closed-chest cardiac massage; and Dr. James Jude, who combined compressions with ventilation. Dr. Peter Safar is most commonly called the “father of CPR.”
When was CPR invented?
The key components of CPR were developed between 1954 and 1960. Mouth-to-mouth resuscitation was demonstrated by Peter Safar in 1956, and closed-chest compressions were proven effective by Kouwenhoven’s team in 1960. Modern CPR, combining both techniques, was formally introduced in 1960 and endorsed by the American Heart Association in 1963.
Who invented the CPR dummy?
The CPR training mannequin “Resusci Anne” (also called CPR Annie) was created by Norwegian toymaker Asmund Laerdal in the early 1960s. Peter Safar influenced Laerdal to design the mannequin, which was modeled after L’Inconnue de la Seine, an unidentified young woman’s death mask from 19th-century Paris. Resusci Anne became the standard tool for teaching CPR worldwide.
Who is the father of CPR?
Dr. Peter Safar (1924-2003), an Austrian-born anesthesiologist, is widely known as the “father of CPR.” He developed the A-B-C approach (Airway, Breathing, Circulation), wrote the foundational textbook on resuscitation, and established the first ICU in the United States.
Has CPR changed since it was invented?
Yes, CPR guidelines are regularly updated. One of the most significant changes came in 2010 when the AHA changed the recommended sequence from A-B-C (Airway, Breathing, Compressions) to C-A-B (Compressions, Airway, Breathing). This change prioritized starting chest compressions immediately. Guidelines also now emphasize hands-only CPR for untrained bystanders and the early use of AEDs.
Prabakar Mahalingam is the Managing Partner at AED Total Solution, a full-service AED program management company. With extensive experience in emergency preparedness and compliance, he leads efforts to help organizations maintain AED readiness, CPR certification tracking, and regulatory compliance.
The information provided is for educational purposes only and does not replace professional medical advice or formal CPR training. Always consult qualified healthcare professionals and obtain proper CPR/AED certification.