By Prabakar Mahalingam, Managing Partner at AED Total Solution. Prabakar is a nationally recognized provider of safety training, products, and proprietary compliance software dedicated to addressing Sudden Cardiac Arrest (SCA). He leads comprehensive AED programs throughout North America.
Key Takeaways: An AED only delivers a shock for two specific heart rhythms: ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT). These shockable rhythms account for the majority of out-of-hospital cardiac arrests where defibrillation can restore a normal heartbeat. Non-shockable rhythms like asystole and pulseless electrical activity (PEA) require CPR and advanced medical intervention instead. Understanding what shockable rhythms are, and how an AED detects them, helps workplace safety managers build effective cardiac emergency response programs.
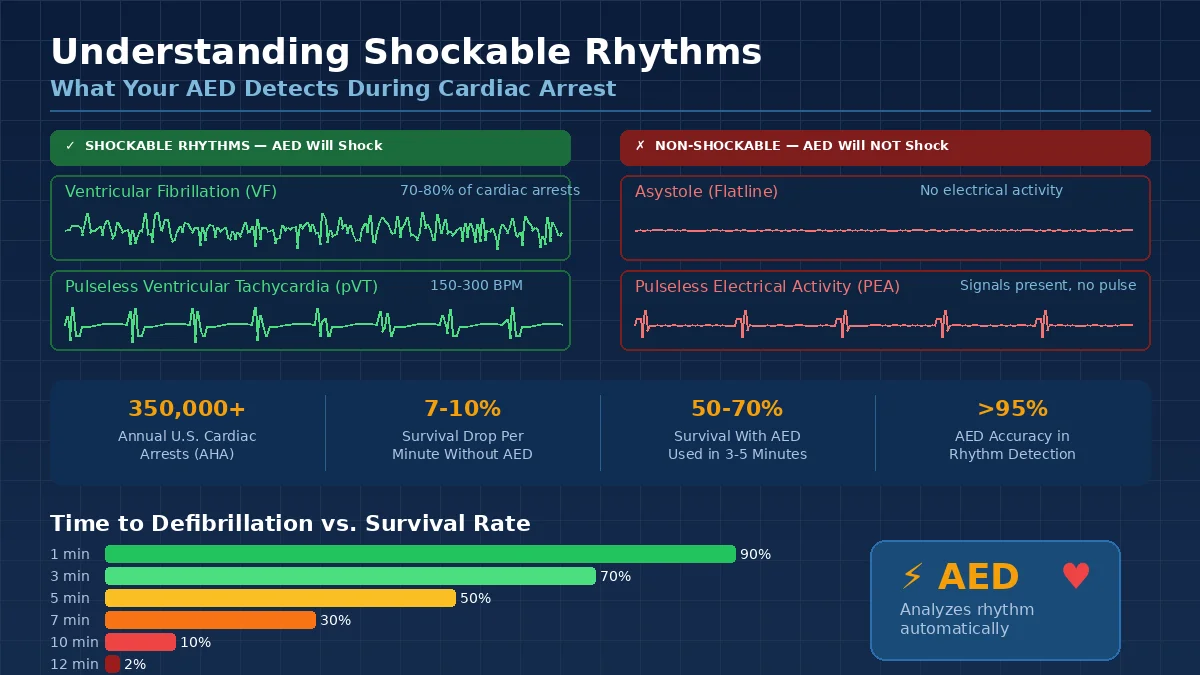
Every year, more than 350,000 people in the United States experience sudden cardiac arrest outside a hospital, according to the American Heart Association. Survival depends on how quickly the right treatment reaches the right person. For workplace safety managers, compliance officers, and facilities leaders, understanding shockable rhythms is not just medical knowledge. It is the foundation of an effective AED program.
An automated external defibrillator does not shock every cardiac arrest victim. The device analyzes the heart’s electrical activity and determines whether the rhythm it detects will respond to a shock. Only two rhythms qualify. This guide explains what those rhythms are, why they matter, and how AEDs make the decision to shock or not.
What Are Shockable Rhythms?
Shockable rhythms are abnormal heart rhythms where the heart’s electrical system has malfunctioned, but there is still electrical activity that a defibrillator can reset. The heart is not pumping blood effectively, but its electrical signals have not completely stopped. A precisely timed electrical shock can interrupt the chaotic signals and give the heart a chance to restart with a normal rhythm.
The American Heart Association identifies two shockable rhythms:
- Ventricular fibrillation (VF or V-fib)
- Pulseless ventricular tachycardia (pVT or V-tach)
Both conditions cause the heart to stop pumping blood. Without treatment, they lead to death within minutes. An AED is specifically designed to detect these two rhythms and deliver an electrical shock to correct them.
How the Heart’s Electrical System Works
To understand why only certain rhythms respond to defibrillation, it helps to know how the heart normally functions.
The heart beats because of an internal electrical system. A natural pacemaker called the sinoatrial (SA) node generates electrical impulses that travel through the heart in a coordinated sequence. These impulses cause the heart’s four chambers (two atria on top, two ventricles on the bottom) to contract in the correct order, pushing blood through the body.
This system operates on three connected functions:
- Electrical: The SA node fires impulses that trigger each heartbeat. If it fails, backup pacemakers in the heart take over.
- Mechanical: The heart muscle contracts in response to electrical signals, squeezing blood out of each chamber.
- Hydraulic: Blood flows through the chambers, picking up oxygen in the lungs and delivering it to every organ.
When the electrical system malfunctions, the mechanical and hydraulic systems fail with it. The heart either quivers uselessly or beats so fast that it cannot fill with blood between contractions. In both cases, blood flow stops.
Ventricular Fibrillation (VF): The Most Common Shockable Rhythm
Ventricular fibrillation is the most frequent cause of sudden cardiac arrest. It accounts for approximately 70% to 80% of initial rhythms detected in out-of-hospital cardiac arrests where the event was witnessed, according to data from the Cardiac Arrest Registry to Enhance Survival (CARES).
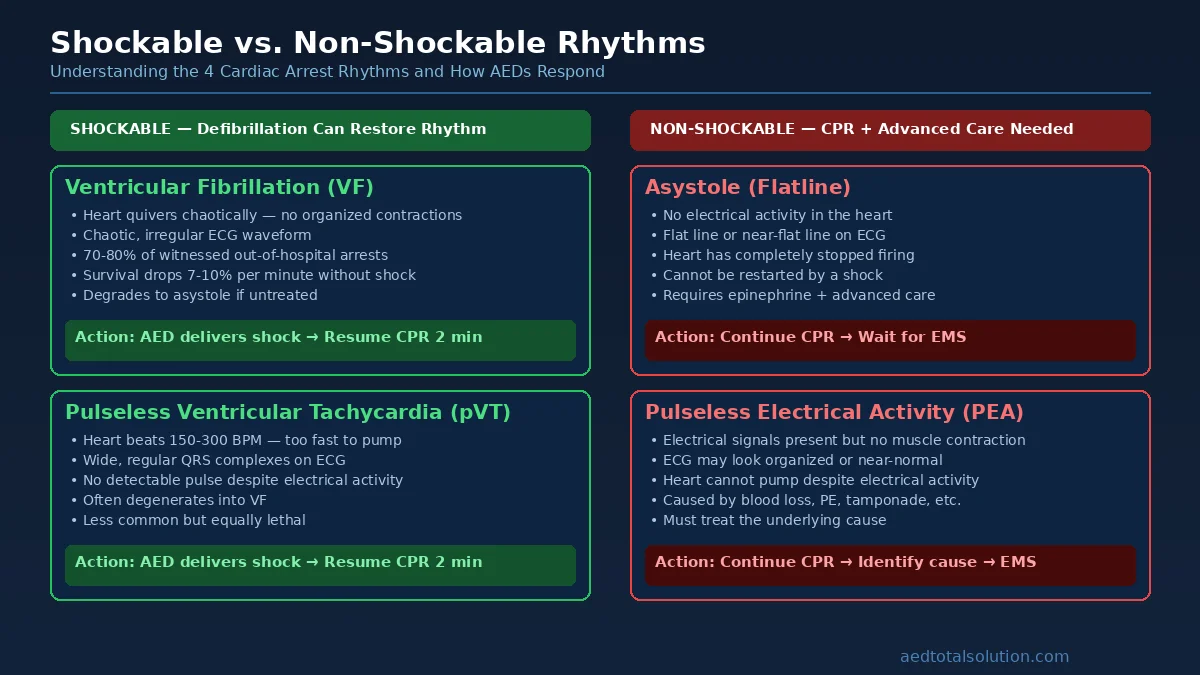
During VF, the ventricles (the heart’s lower pumping chambers) receive chaotic, disorganized electrical signals. Instead of contracting in a coordinated rhythm, the muscle fibers quiver rapidly and randomly. On an electrocardiogram (ECG), VF appears as a jagged, irregular waveform with no recognizable pattern.
What happens during VF:
- The ventricles quiver at 300 to 500 disorganized impulses per minute
- No blood is pumped to the brain, lungs, or other organs
- The person collapses, becomes unresponsive, and stops breathing normally
- Without intervention, VF deteriorates into asystole (flatline) within minutes
Why defibrillation works for VF: The electrical shock passes through the heart muscle and depolarizes (resets) the cells simultaneously. This momentary pause in all electrical activity gives the SA node an opportunity to re-establish its normal rhythm. Think of it as clearing a traffic jam by stopping all vehicles at once, then letting them restart in an orderly sequence.
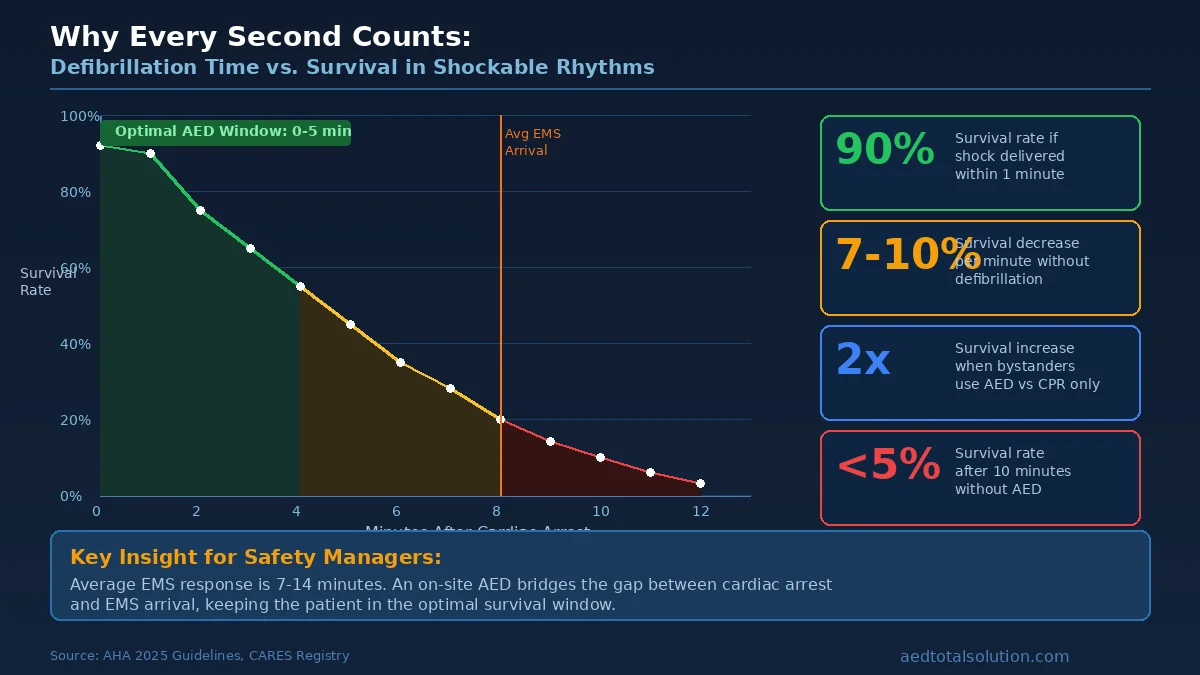
The critical factor is time. Research published in the journal Circulation shows that for every minute defibrillation is delayed, the chance of survival decreases by 7% to 10%. When an AED delivers a shock within the first three to five minutes of VF, survival rates can exceed 50%.
Pulseless Ventricular Tachycardia (pVT): The Second Shockable Rhythm
Pulseless ventricular tachycardia occurs when the ventricles beat extremely fast, typically between 150 and 300 beats per minute, but fail to generate a detectable pulse. The electrical signals are more organized than in VF, but the heart rate is so rapid that the ventricles cannot fill with blood between beats.
On an ECG, pVT shows wide, regular QRS complexes at a rapid rate. Unlike VF’s chaotic waveform, pVT has a recognizable, repeating pattern, but the speed prevents effective pumping.
What happens during pVT:
- The ventricles contract too rapidly to fill with blood
- Cardiac output drops to near zero
- The person loses consciousness and has no palpable pulse
- Without treatment, pVT frequently degenerates into VF
Why defibrillation works for pVT: Similar to VF, the electrical shock interrupts the rapid, abnormal circuit driving the tachycardia. Once the circuit is broken, the heart’s natural pacemaker can reassert control and restore a normal rate and rhythm.
pVT is less common than VF as an initial cardiac arrest rhythm, but it is equally life-threatening. AEDs are programmed to detect both conditions because the treatment, prompt defibrillation combined with high-quality CPR, is the same for both.
Non-Shockable Rhythms: Why AEDs Sometimes Say “No Shock Advised”
Not every cardiac arrest involves a shockable rhythm. Two non-shockable rhythms require different treatment:
Asystole (Flatline)
Asystole means the heart has no electrical activity at all. There is no heartbeat, no quivering, and no signal to reset. On an ECG, asystole appears as a flat line or a nearly flat line with minimal electrical noise.
An AED will not shock asystole because there is no electrical activity to reset. Defibrillation works by interrupting chaotic signals. When there are no signals, a shock cannot help. This is why the dramatic movie scene of shocking a flatline back to life is medically inaccurate.
Treatment for asystole focuses on high-quality CPR, epinephrine (administered by paramedics), and identifying reversible causes.
Pulseless Electrical Activity (PEA)
PEA occurs when the heart’s electrical system generates signals that appear organized on an ECG, but the heart muscle does not respond with effective contractions. The “electrical” part is present; the “mechanical” part has failed.
An AED will not shock PEA because the electrical rhythm may look normal on the monitor. The problem is not with the electrical signals themselves but with the heart’s ability to contract. Common causes include severe blood loss, tension pneumothorax, cardiac tamponade, and massive pulmonary embolism.
Treatment for PEA requires high-quality CPR, advanced life support medications, and rapid identification and treatment of the underlying cause.
Quick Reference: Shockable vs. Non-Shockable Rhythms
| Rhythm | Shockable? | What the AED Does | What You Should Do |
|---|---|---|---|
| Ventricular Fibrillation (VF) | Yes | Advises shock | Clear the patient, deliver shock, resume CPR |
| Pulseless Ventricular Tachycardia (pVT) | Yes | Advises shock | Clear the patient, deliver shock, resume CPR |
| Asystole | No | Says “No shock advised” | Continue high-quality CPR, call 911 |
| Pulseless Electrical Activity (PEA) | No | Says “No shock advised” | Continue high-quality CPR, call 911 |
One of the most common concerns among workplace safety managers is whether untrained employees can safely use an AED. The answer is yes, and understanding how the technology works explains why.
The Analysis Process
When you place AED electrode pads on a person’s bare chest, the device begins analyzing the heart’s electrical signals through a process similar to a simplified electrocardiogram. Here is what happens:
- Signal detection: The electrode pads pick up the heart’s electrical activity through the skin. The AED’s processor filters out noise from muscle movement, interference, and other sources.
- Rhythm classification: A sophisticated algorithm analyzes the signal’s frequency, amplitude, and regularity. The software compares the detected pattern against its database of known rhythms to determine if VF or pVT is present.
- Shock decision: If the AED detects a shockable rhythm, it charges its capacitor and prompts the rescuer to deliver the shock. If it detects a non-shockable rhythm, it advises “No shock” and instructs the rescuer to continue CPR.
Why You Cannot Accidentally Shock Someone Who Does Not Need It
Modern AEDs have a specificity rate above 95%, meaning they are highly accurate at identifying non-shockable rhythms and withholding shocks. The device will not charge or deliver a shock unless its algorithm confirms a shockable rhythm. This built-in safety means:
- A bystander cannot accidentally shock a conscious person. If someone has a normal heart rhythm, the AED will say “No shock advised.”
- The AED will not shock asystole. Despite what movies suggest, the device knows the difference between a chaotic rhythm it can fix and a flatline it cannot.
- Semi-automatic AEDs require a button press. Even after detecting a shockable rhythm, most AEDs prompt the rescuer to press a button. Fully automatic models deliver the shock after a countdown and warning.
This technology is the reason AEDs are approved for use by the general public without medical training. The device makes the clinical decision. The rescuer’s job is to place the pads correctly, stand clear when prompted, and perform CPR between analysis cycles.
For guidance on correct electrode placement, see our AED pad placement guide.
Why Every Minute Counts: The Time Factor in Shockable Rhythms
The relationship between time and survival in shockable rhythms is not linear. It is a steep decline.
According to the American Heart Association’s 2025 Guidelines Update:
- Within 1 minute: Survival rates can be as high as 90% if defibrillation is immediate
- 3 to 5 minutes: Survival rates range from 50% to 70% with bystander CPR and early AED use
- After 10 minutes: Survival rates drop below 5% without defibrillation
- Every additional minute without defibrillation reduces survival by approximately 7% to 10%
These numbers explain why workplace AED programs are not optional for organizations serious about employee safety. Emergency medical services (EMS) average response times range from 7 to 14 minutes depending on location. In many cases, that is too late for a shockable rhythm.
CPR alone can maintain some blood flow to the brain and vital organs, but it does not convert a shockable rhythm back to normal. Only defibrillation does that. CPR buys time; the AED delivers the definitive treatment.
Research from the CARES registry shows that when bystanders use an AED before EMS arrives, survival rates more than double compared to CPR alone. For workplace safety managers, this data makes the business case clear: having an accessible, maintained AED on-site is the single most impactful step you can take to save a life during sudden cardiac arrest.
Why Workplace AED Programs Matter
Understanding shockable rhythms is only valuable if your organization is prepared to act on that knowledge. An effective workplace AED program connects the science to practical readiness.
The Workplace Risk
The Occupational Safety and Health Administration (OSHA) reports approximately 10,000 cardiac arrests in U.S. workplaces each year. Many occur in seemingly low-risk environments like offices, retail spaces, and warehouses. Sudden cardiac arrest does not discriminate by industry, age, or fitness level.
Workplaces present a unique advantage: there are usually other people nearby who can respond immediately. An AED on the wall and employees who know where it is can mean the difference between a five-minute response and a fifteen-minute wait for paramedics.
What a Complete AED Program Includes
Placing an AED on the wall is a start, but a compliant, effective program requires more:
- Strategic placement: AEDs should be accessible within a two-minute walking distance from any point in the facility. High-traffic areas, lobbies, fitness centers, and cafeterias are priority locations.
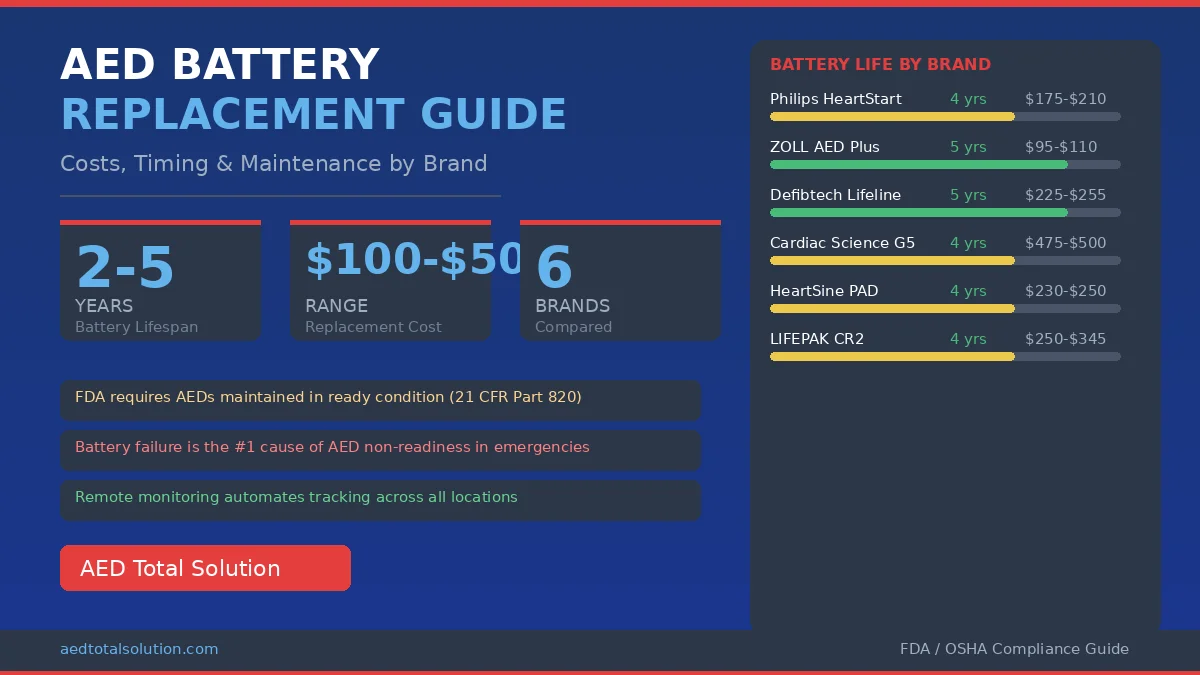
- Regular inspections: AED batteries and electrode pads have expiration dates. Monthly visual inspections verify the device is ready. Read our AED inspection guide for a complete checklist.
- Staff awareness training: Employees do not need to be cardiologists. They need to know where the AED is, how to turn it on, and that the device guides them through every step. Visit our how to use an AED page for a step-by-step walkthrough.
- Compliance documentation: Many states require AED registration, maintenance records, and designated AED coordinators. Our AED program management service handles this entirely.
- Ongoing monitoring: Remote monitoring technology can alert your team when a device needs attention, a battery is low, or pads are nearing expiration.
The Legal Landscape
Good Samaritan laws in all 50 states provide legal protection for people who use an AED in good faith during an emergency. These protections extend to both the rescuer and the organization that provides the AED, as long as the device is properly maintained and the user acts in good faith.
Many states now require AEDs in specific settings including schools, fitness centers, government buildings, and large commercial facilities. Maintaining a compliant AED program is both a safety imperative and a regulatory requirement.
Frequently Asked Questions About Shockable Rhythms
What are the two shockable rhythms?
The two shockable rhythms are ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT). These are the only cardiac arrest rhythms that respond to defibrillation from an AED. Both involve electrical malfunction in the heart’s ventricles that prevents effective blood pumping.
Can an AED shock a normal heart rhythm?
No. AEDs are designed to analyze heart rhythm before advising a shock. If the heart has a normal rhythm, the AED will display “No shock advised” and will not allow a shock to be delivered. The device’s algorithm is highly accurate at distinguishing shockable from non-shockable rhythms.
Why does an AED say “No shock advised” during cardiac arrest?
This message means the AED detected a non-shockable rhythm, either asystole (no electrical activity) or pulseless electrical activity (PEA). In these cases, defibrillation will not help. Continue performing high-quality CPR and wait for advanced medical personnel to arrive.
Is asystole a shockable rhythm?
No. Asystole (flatline) is not a shockable rhythm. There is no electrical activity for a defibrillator to reset. Treatment for asystole requires high-quality CPR and advanced cardiac life support (ACLS) medications like epinephrine, administered by trained medical professionals.
What is the difference between VF and pVT?
Ventricular fibrillation produces chaotic, disorganized electrical activity where the heart quivers without pumping. Pulseless ventricular tachycardia produces rapid but more organized electrical signals, though the heart beats too fast to pump blood effectively. Both are shockable and both are immediately life-threatening. An AED treats both the same way: with a controlled electrical shock.
Do I need medical training to use an AED?
No. AEDs are designed for use by anyone, including people with no medical training. The device provides step-by-step voice and visual instructions. It analyzes the heart rhythm automatically and will only allow a shock if one is medically appropriate. The AED makes the clinical decision; you simply follow the prompts.
AED Total Solution provides full-service AED program management, including device placement consulting, compliance tracking, remote monitoring, and ongoing maintenance. To learn more about building a workplace AED program, explore our AED products or rental programs, or call us at (855) 263-7772.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always follow your organization’s emergency protocols and call 911 immediately when someone experiences cardiac arrest. AED Total Solution recommends that all employees complete basic CPR and AED training through an accredited provider.