Both cardioversion and defibrillation use electrical energy to correct dangerous heart rhythms, but they are not interchangeable. Understanding the difference between these two procedures is critical for healthcare professionals, safety officers, and anyone responsible for workplace emergency preparedness.
This guide breaks down how synchronized cardioversion and defibrillation work, when each procedure is appropriate, how AEDs perform defibrillation, and what this means for your organization’s cardiac emergency response plan.
What Is Cardioversion?
Cardioversion is a medical procedure that restores a normal heart rhythm in patients experiencing certain types of arrhythmias, or irregular heartbeats. It is most commonly used for conditions like atrial fibrillation (AFib), atrial flutter, and supraventricular tachycardia (SVT), where the heart beats irregularly but still maintains some organized electrical activity.
There are two types of cardioversion:
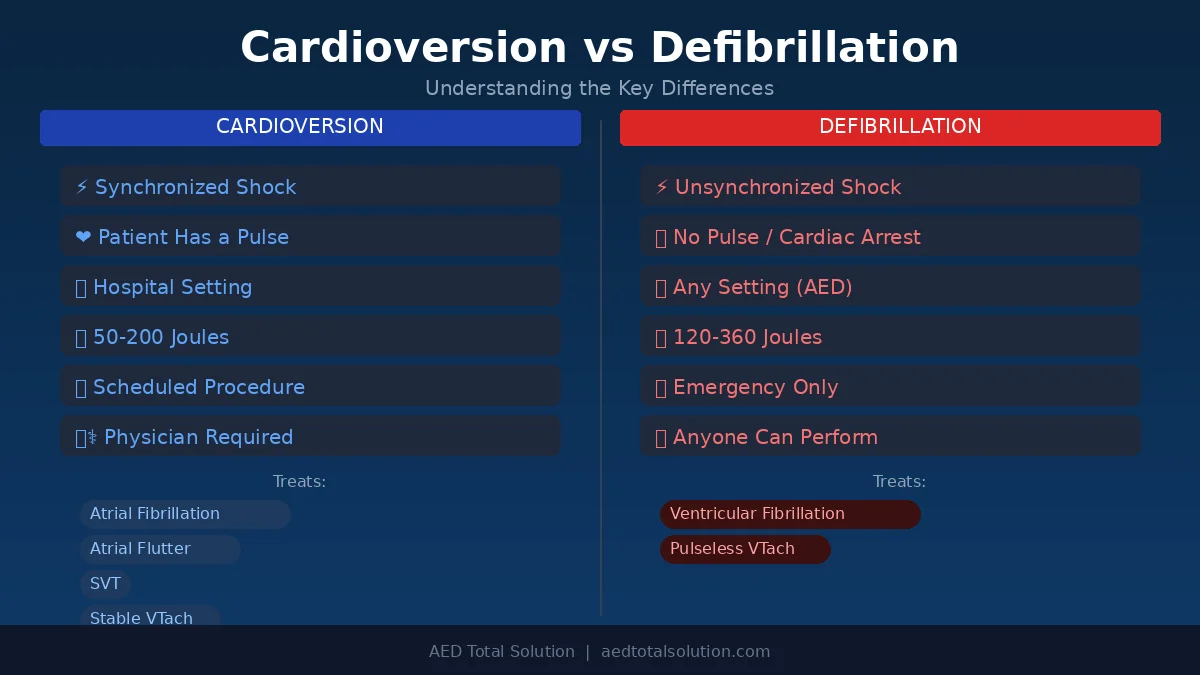
- Electrical cardioversion (synchronized cardioversion): A controlled electrical shock is delivered through electrode pads placed on the patient’s chest. The shock is precisely timed, or “synchronized,” to the R-wave of the heart’s electrical cycle. This timing prevents the shock from hitting during the vulnerable T-wave period, which could trigger a more dangerous rhythm like ventricular fibrillation.
- Chemical (pharmacologic) cardioversion: Antiarrhythmic medications are administered intravenously or orally to restore normal rhythm without electrical shock. Common medications include amiodarone, flecainide, and ibutilide.
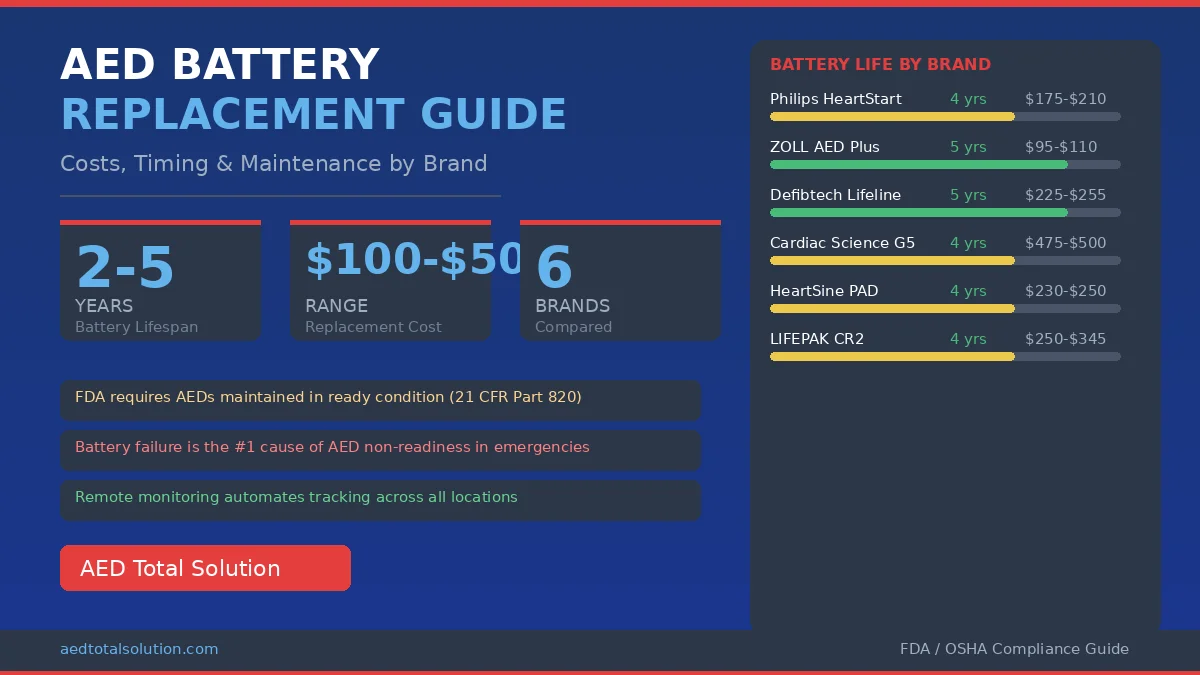
Electrical cardioversion is typically a scheduled, elective procedure performed in a hospital or clinical setting. Patients are sedated, and the procedure is closely monitored by a cardiologist or electrophysiologist. The energy levels used are generally lower than defibrillation, often starting at 50 to 100 joules for atrial fibrillation and adjusted based on the patient’s response.
What Is Defibrillation?
Defibrillation is an emergency procedure that delivers a high-energy, unsynchronized electrical shock to the heart. It is used when a patient is in cardiac arrest caused by a life-threatening arrhythmia, specifically ventricular fibrillation (VFib) or pulseless ventricular tachycardia (VTach).
During ventricular fibrillation, the heart’s electrical system becomes completely chaotic. The ventricles quiver instead of contracting effectively, and blood stops flowing to the brain and vital organs. Without immediate intervention, this condition is fatal within minutes.
Defibrillation works by depolarizing all the heart muscle cells simultaneously. This brief electrical “reset” stops the chaotic activity and gives the heart’s natural pacemaker, the sinoatrial (SA) node, the opportunity to re-establish a normal, coordinated rhythm.
Key characteristics of defibrillation include:
- Unsynchronized shock delivery: Because ventricular fibrillation produces no organized electrical pattern, the defibrillator does not need to time the shock to the cardiac cycle. It delivers the shock as soon as it is charged and activated.
- Higher energy levels: Defibrillation typically uses 120 to 360 joules (depending on whether the device is biphasic or monophasic), significantly more energy than synchronized cardioversion.
- Emergency application: Defibrillation is performed on patients who are unresponsive, not breathing normally, and have no pulse. Every minute without defibrillation reduces the chance of survival by approximately 7 to 10 percent.
How AEDs Perform Defibrillation
An automated external defibrillator (AED) is a portable device designed to deliver defibrillation quickly and effectively, even by bystanders with no medical training. AEDs are specifically built for the emergency use case: they analyze the heart’s rhythm and determine whether a shock is needed.
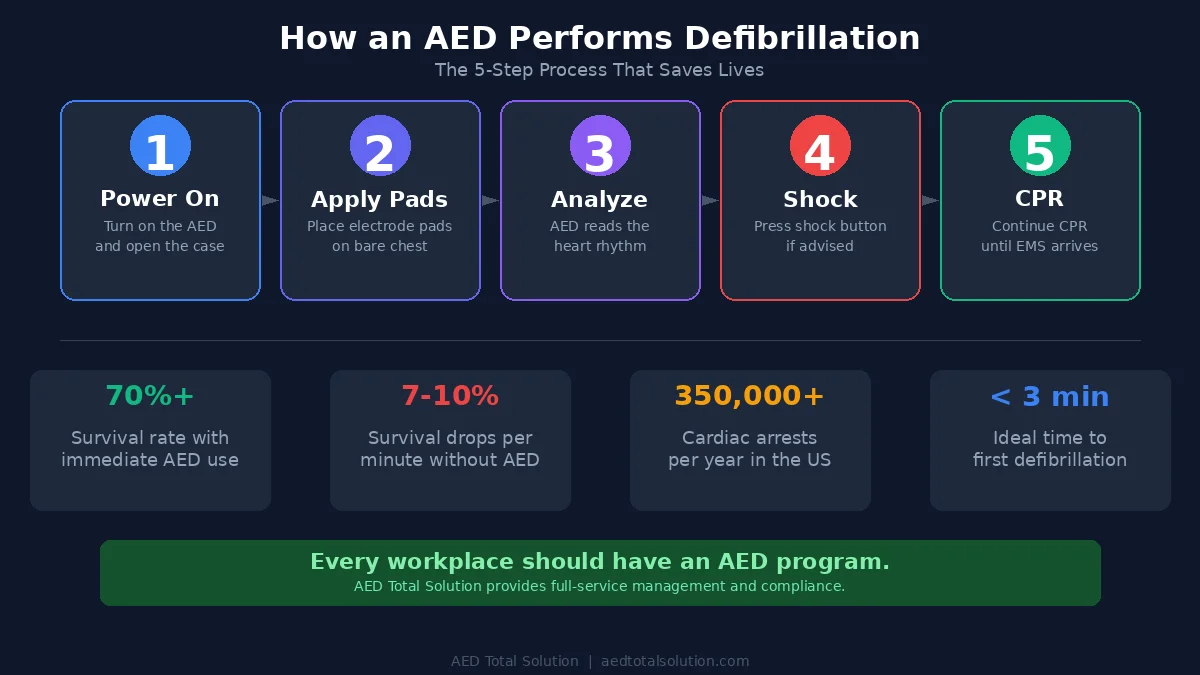
Here is how an AED works step by step:
- Power on and apply pads: The rescuer turns on the AED and places adhesive electrode pads on the patient’s bare chest (one pad on the upper right chest, one on the lower left side).
- Heart rhythm analysis: The AED’s built-in processor analyzes the patient’s heart rhythm through the electrode pads. It uses algorithms to detect shockable rhythms, specifically ventricular fibrillation and pulseless ventricular tachycardia.
- Shock advisory: If a shockable rhythm is detected, the AED instructs the rescuer to deliver a shock. If the rhythm is not shockable (such as asystole or pulseless electrical activity), the AED will not allow a shock to be delivered.
- Shock delivery: The rescuer presses the shock button (or, in fully automatic AEDs, the shock is delivered automatically after a countdown). The device delivers a controlled, biphasic shock at an appropriate energy level.
- Post-shock guidance: After the shock, the AED prompts the rescuer to continue CPR and re-analyzes the rhythm at regular intervals.
Modern AEDs are designed with safety mechanisms that prevent inappropriate shocks. They only deliver energy when they detect a shockable rhythm, making them safe for use by trained and untrained individuals alike.
The presence of AEDs in workplaces, schools, and public spaces is a key component of sudden cardiac arrest survival. Studies show that immediate AED use, combined with CPR, can increase survival rates to over 70 percent when applied within the first few minutes of cardiac arrest.
Synchronized Cardioversion vs Defibrillation: Key Differences
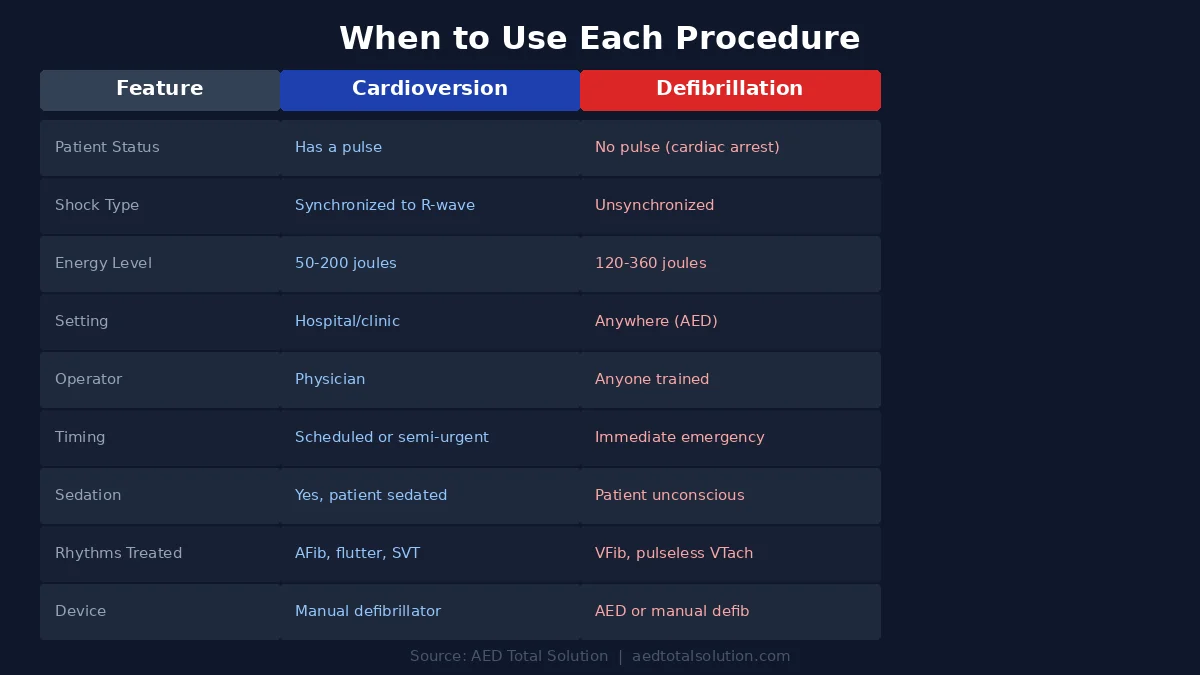
The fundamental difference between cardioversion and defibrillation comes down to timing, energy, and clinical context. Here is a side-by-side comparison:
| Feature | Synchronized Cardioversion | Defibrillation |
|---|---|---|
| Shock timing | Synchronized to the R-wave of the cardiac cycle | Unsynchronized; delivered immediately |
| Patient condition | Has a pulse; hemodynamically unstable or symptomatic arrhythmia | No pulse; cardiac arrest (VFib or pulseless VTach) |
| Typical energy level | 50–200 joules (starting lower) | 120–360 joules (biphasic/monophasic) |
| Setting | Hospital or clinical environment with sedation | Any setting; emergency field use with AEDs |
| Arrhythmias treated | Atrial fibrillation, atrial flutter, SVT, stable ventricular tachycardia | Ventricular fibrillation, pulseless ventricular tachycardia |
| Who performs it | Physician, cardiologist, or trained medical staff | Anyone (with AED); paramedics, EMTs, bystanders |
| Device used | Manual defibrillator/cardioverter in synchronized mode | AED or manual defibrillator in unsynchronized mode |
| Patient consciousness | Typically sedated before procedure | Unresponsive/unconscious |
| Urgency | Scheduled or semi-urgent | Immediate; life or death |
When Is Cardioversion Used?
Cardioversion is appropriate when a patient has an organized but abnormal heart rhythm and still has a pulse. Common clinical scenarios include:
- Atrial fibrillation (AFib): The most common arrhythmia, where the atria beat chaotically. Cardioversion may be recommended when medications fail to restore normal rhythm or when the patient experiences significant symptoms.
- Atrial flutter: A rapid but organized atrial rhythm. Cardioversion is often highly effective for this condition, sometimes requiring as little as 50 joules.
- Supraventricular tachycardia (SVT): A rapid heart rate originating above the ventricles. If vagal maneuvers and medications do not work, synchronized cardioversion is the next step.
- Stable ventricular tachycardia with a pulse: When VTach produces symptoms but the patient still has a pulse and blood pressure, synchronized cardioversion is preferred over defibrillation.
Before performing electrical cardioversion, physicians typically order blood tests, an echocardiogram, and may prescribe blood thinners to reduce the risk of stroke from blood clots that can form during prolonged arrhythmias.
When Is Defibrillation Used?
Defibrillation is reserved for cardiac arrest scenarios where the patient has no effective heartbeat. The two shockable cardiac arrest rhythms are:
- Ventricular fibrillation (VFib): The ventricles quiver chaotically, producing no effective cardiac output. This is the most common initial rhythm in sudden cardiac arrest and the most responsive to defibrillation.
- Pulseless ventricular tachycardia (pVTach): The ventricles beat very rapidly without producing a pulse. While still organized, this rhythm does not effectively pump blood and degenerates into VFib without treatment.
The chain of survival for sudden cardiac arrest follows these critical steps:
- Recognize cardiac arrest and call 911
- Begin CPR immediately
- Use an AED as soon as one is available
- Advanced medical care by EMS professionals
Time is the most critical factor. For every minute that passes without defibrillation, the chance of survival drops significantly. This is why having accessible AEDs in your facility and trained responders is essential for any organization.
Why the Distinction Matters for Workplace Safety
For safety officers, facilities managers, and compliance directors, understanding the difference between cardioversion and defibrillation has practical implications:
- AEDs perform defibrillation, not cardioversion. The AED units deployed in your workplace are designed exclusively for emergency defibrillation. They cannot and should not be used for synchronized cardioversion, which requires a medical setting and physician oversight.
- AED training should emphasize when to use the device. Employees should understand that AEDs are for unresponsive individuals with no pulse, not for someone experiencing heart palpitations or other non-emergency cardiac symptoms.
- AED readiness is a compliance priority. Many states require certain businesses and organizations to maintain AED programs. Regular inspections, pad and battery replacement, and staff training are all part of maintaining a compliant AED program.
- Medical emergencies require clear protocols. Your workplace emergency action plan should distinguish between cardiac arrest (use AED, call 911) and other cardiac events (call 911, do not use AED).
Frequently Asked Questions
What is the main difference between cardioversion and defibrillation?
The main difference is timing and patient condition. Cardioversion delivers a synchronized electrical shock to a patient who has a pulse but an abnormal heart rhythm. Defibrillation delivers an unsynchronized shock to a patient in cardiac arrest with no pulse, specifically those in ventricular fibrillation or pulseless ventricular tachycardia.
Can an AED perform cardioversion?
No. AEDs are designed exclusively for defibrillation. They deliver unsynchronized shocks to treat cardiac arrest caused by shockable rhythms (VFib and pulseless VTach). Synchronized cardioversion requires a manual defibrillator operated by trained medical professionals in a clinical setting.
Is defibrillation more dangerous than cardioversion?
Both procedures carry risks, but the context is different. Defibrillation is an emergency intervention where the alternative is death. The risk of not defibrillating far outweighs any risk from the shock itself. Cardioversion is performed on patients with a pulse under controlled conditions, and risks include temporary skin irritation and rare complications like blood clots or stroke.
When should I use an AED vs. calling for cardioversion?
Use an AED when someone collapses, is unresponsive, and is not breathing normally. This suggests cardiac arrest requiring immediate defibrillation. Cardioversion is a medical decision made by a physician for patients with a pulse who have sustained arrhythmias. If someone is conscious and experiencing heart rhythm problems, call 911 and let medical professionals decide on treatment.
How much energy does an AED deliver compared to cardioversion?
AEDs typically deliver between 120 and 200 joules using biphasic waveform technology. Synchronized cardioversion usually starts at lower energy levels, around 50 to 100 joules for atrial fibrillation, and may be increased if the initial shock is unsuccessful.
Does every workplace need an AED?
While not every state mandates AEDs in all workplaces, having an AED program is strongly recommended by OSHA, the American Heart Association, and other safety organizations. Sudden cardiac arrest can happen anywhere, and survival rates drop dramatically without immediate access to defibrillation. Many states have specific AED requirements for certain facility types.
Conclusion
Cardioversion and defibrillation both use electrical energy to address heart rhythm disorders, but they serve fundamentally different purposes. Cardioversion is a controlled, medical procedure for patients with a pulse and an abnormal rhythm. Defibrillation is an emergency intervention for patients in cardiac arrest.
For workplace safety teams, the takeaway is clear: AEDs are defibrillation devices designed for cardiac arrest emergencies. Having a well-maintained AED program, trained staff, and clear emergency protocols can mean the difference between life and death when sudden cardiac arrest strikes.
If your organization needs help establishing or managing an AED program, AED Total Solution provides full-service AED program management, from device selection and deployment to ongoing compliance monitoring and staff training. Contact us to learn how we can help keep your workplace prepared. Our AED rental program makes it easy to equip your facility with FDA-approved defibrillators starting at $45/month.
Written by Prabakar Mahalingam, Managing Partner at AED Total Solution and recognized national provider of safety training, products, and proprietary compliance software dedicated to addressing Sudden Cardiac Arrest.